Key Takeaways
- Malware infections remain the leading attack type from 2025 to 2026, affecting 48% of organizations that experienced an incident.
- Remote access exploitation increased to 38% in 2026, up from 28% in 2025, making it one of the fastest-growing threat vectors affecting healthcare and medical devices.
- Ransomware targeting device operations affected 32% of impacted organizations, with recovery times extending well beyond the immediate downtime window.
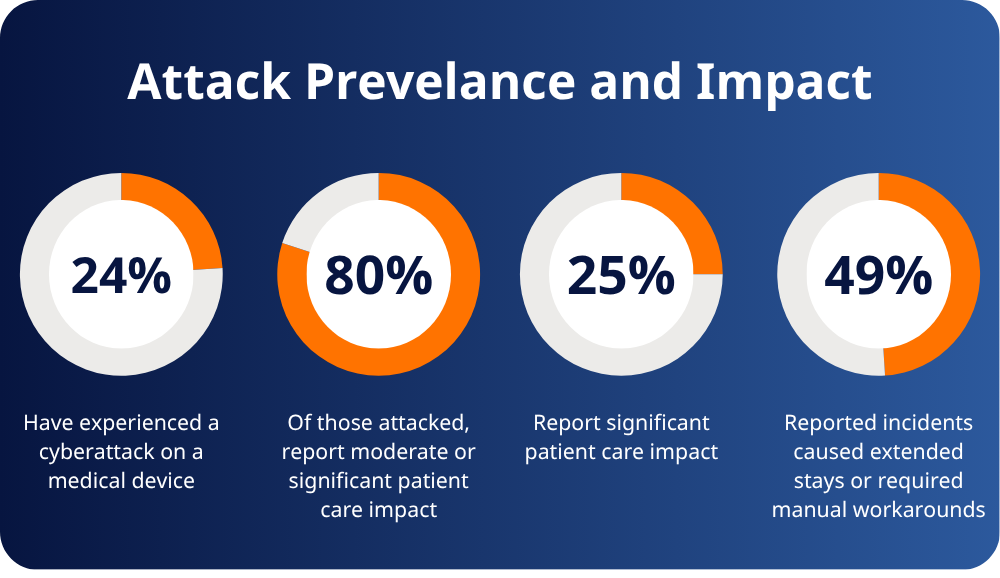
- 80% of organizations that experienced an attack reported a moderate or significant impact on patient care.
When a medical device goes down during a cyberattack, patient care is directly affected. Procedures get delayed, staff revert to manual workarounds, and patients wait longer for treatment. In 2026, 80% of healthcare organizations that experienced an attack affecting a medical device reported moderate or significant impact on patient care.
RunSafe Security’s 2026 Medical Device Cybersecurity Index asked 551 healthcare professionals across the U.S., UK, and Germany to identify the medical device vulnerabilities driving those incidents. The data reveals eight distinct attack types, how frequently each is occurring, and where the threat profile is shifting compared to 2025. Here is what healthcare security teams and device manufacturers are actually up against.
1. Malware Infections Requiring Device Quarantine (48%)
Malware remains the most frequently reported attack type, cited by 48% of organizations that experienced an incident. While that figure has edged down slightly from 51% in 2025, the operational consequence is unchanged: infected devices must be isolated, often pulling critical equipment out of service at the worst possible time.
Malware targeting medical devices is rarely opportunistic. Campaigns tend to be deliberate, designed to force quarantine of specific device categories—imaging systems, monitoring equipment, infusion pumps—and trigger cascading disruption across the care environment. In some cases, attackers wipe firmware or corrupt system files, requiring full reinstallation before devices can return to service. The disruption extends well past the initial incident.
What it means operationally: Organizations that lack network segmentation between clinical and administrative systems are especially exposed. Malware introduced through a non-clinical endpoint can reach device networks quickly if east-west movement is not restricted. Detecting infections on devices running legacy or unsupported operating systems that cannot run traditional endpoint protection requires dedicated monitoring tools designed for clinical environments.
2. Network Intrusions Requiring Device Isolation (41%)
Network intrusions were reported by 41% of affected organizations, and they carry a distinct risk profile from malware. Network intrusions often go undetected for extended periods. Attackers gain access through poorly segmented networks, default credentials, or outdated communication protocols, then move laterally before triggering any visible disruption.
Once inside a device network, adversaries can establish persistent footholds, capture data in transit, or manipulate device configurations without triggering alarms. The intrusion may predate the identified incident by weeks or months. When it is finally discovered, isolation is the immediate response—but the question of what happened during the undetected window often remains open.
What it means operationally: The 12-hour average recovery window reported in the 2026 Index understates the full exposure period for network intrusions. Organizations should assume device network visibility is incomplete and prioritize continuous monitoring tools that detect anomalous behavior at the device level, not just at the network perimeter.
3. Remote Access Exploitation (38%)
Remote access exploitation has become one of the fastest-growing attack vectors in medical device security. Reported by 38% of affected organizations in 2026, up from 28% in 2025, the increase tracks directly with the expanding remote access footprint of connected clinical devices—remote maintenance, vendor diagnostics, software updates, and clinical monitoring all depend on it.
Attackers exploit default or reused credentials on remote maintenance tools, unsecured VPN configurations, and vendor accounts with excessive privileges. Once inside, they have the same level of access as an authorized technician. The growing adoption of telehealth infrastructure and remote device management has expanded the attack surface significantly, and threat actors targeting healthcare have noticed.
What it means operationally: Every vendor with remote access to a device is a potential entry point. Organizations should audit active remote access accounts, enforce least-privilege access, require multi-factor authentication for all remote sessions, and ensure vendor access is time-limited and logged. The devices most at risk are those with persistent, always-on remote access enabled by default.
4. Ransomware Affecting Device Operations (32%)
Ransomware targeting medical device operations was reported by 32% of affected organizations. Unlike ransomware that encrypts files and demands payment to restore data, device-targeted ransomware attacks availability directly.
Attackers know that clinical operations cannot pause. Locking operators out of imaging systems, surgical robots, or monitoring equipment creates immediate pressure that IT-focused ransomware does not. Organizations facing device-level ransomware often have no fallback: the affected equipment cannot be substituted, and manual workarounds for complex diagnostic or surgical systems are limited at best.
What it means operationally: Ransomware targeting devices typically arrives through the same vectors as other attacks—compromised credentials, unpatched vulnerabilities, and lateral movement from an already-infected network. The controls that reduce exposure are the same ones that apply broadly: network segmentation to limit lateral movement, strict access controls to reduce the blast radius of a compromised account, and a tested incident response plan that accounts for device-level outages specifically. Organizations that have not mapped their clinical dependencies—which devices, if taken offline, create the most immediate patient care risk—are poorly positioned to respond when the pressure is on.
5. Vendor-Identified Vulnerabilities Requiring Urgent Patching (32%)
Vendor disclosures requiring urgent response were cited by 32% of affected organizations—a reminder that not all incidents originate with an active attack. When a manufacturer identifies a critical vulnerability in a device already deployed at scale across a health system, the response burden falls on the healthcare organization.
The challenge is that patching medical devices is rarely straightforward. Regulatory approval requirements, clinical downtime constraints, and devices running unsupported operating systems can all prevent timely remediation. Organizations without a clear process for triaging and applying vendor patches under time pressure are often left managing exposure for longer than the disclosure timeline assumes.
What it means operationally: The 2026 Index found that 38% of organizations are occasionally or frequently unable to patch devices in active use. For these organizations, vendor disclosures create a window of known, unmitigated exposure. Runtime exploit prevention—which operates at the binary level and does not require patches—is one of the few controls that can defend devices that cannot be patched regularly or easily.
6. Data Exfiltration from Connected Devices (21%)
Data exfiltration from connected devices was reported by 21% of affected organizations. Medical devices increasingly store or transmit patient data—diagnostic results, imaging results, physiological monitoring data—making them targets not just for operational disruption but also for data theft.
Exfiltration from devices differs from traditional healthcare data breaches in that the device itself is the collection point. Attackers who have established persistent access within a device network can extract data over extended periods, often without triggering alerts associated with large-volume file transfers from IT systems.
What it means operationally: Device data flows are often not monitored with the same rigor as IT network traffic. Organizations should map what data each connected device stores or transmits, verify that encryption is enforced in transit, and include device-level data flows in their broader data loss prevention programs.
7. Supply Chain Compromises (18%)
Supply chain compromises were cited by 18% of affected organizations—a figure that likely understates the true exposure, as these attacks are among the hardest to detect. Vulnerabilities introduced through third-party software components, firmware libraries, or hardware embedded in devices can persist undetected through procurement, deployment, and years of clinical use.
The Log4j compromise demonstrated at scale how a single upstream vendor can become an entry point across thousands of downstream organizations. In the medical device context, the equivalent risk comes from third-party software components embedded in device firmware, often sourced from vendors with limited visibility into their own software supply chains.
What it means operationally: This is the finding that makes Software Bill of Materials (SBOM) adoption consequential rather than merely compliant. An SBOM that is actively reviewed—not just requested and filed—gives organizations visibility into the third-party components in their devices and a mechanism for tracking when those components are implicated in newly disclosed vulnerabilities. The 35% of healthcare buyers in the 2026 Index who say they will not consider a device without an SBOM are responding, in part, to exactly this risk.
8. Memory-Based Attacks (14%)
Memory-based attacks were reported by 14% of affected organizations, making them the least frequently cited vector in the 2026 Index. They are also among the most technically sophisticated and the hardest to detect with conventional security tools.
Memory-based attacks exploit vulnerabilities in device software at the binary level—buffer overflows, use-after-free errors, and similar flaws that allow attackers to execute arbitrary code without leaving artifacts that signature-based detection can identify. Devices built on C and C++ codebases, which describe the majority of medical device software, carry this exposure by default. The vulnerabilities often predate the device’s deployment by years and are never patched because they are never found.
What it means operationally: Traditional patching cannot address memory-based vulnerabilities that have not been identified. Runtime exploit prevention technologies work differently—they harden the binary itself, making memory-based exploitation significantly harder regardless of whether the underlying vulnerability has been disclosed. For devices that cannot be patched or replaced, this is a meaningful form of protection rather than a deferred one.
The 2026 attack data tells a consistent story. Attacks on medical devices are more frequent, more harmful to patients, and more varied in their techniques than they were a year ago. The vectors that are growing fastest—remote access exploitation in particular—reflect how devices are being used and maintained, not just how they were designed. Security strategies built around procurement and patching alone are not sufficient for the installed base of devices already in clinical use. The organizations making progress are the ones deploying controls that work on the devices they have, not just the ones they plan to buy.
Download the full 2026 Medical Device Cybersecurity Index for complete survey findings, incident data, and procurement trends.
Learn more about how RunSafe Security’s runtime protection and SBOM capabilities help manufacturers and health systems address the vulnerabilities that patching cannot reach.